Clinical Guide

Recognizing and Understanding Obsessive-Compulsive Disorder: A Guide for Professionals
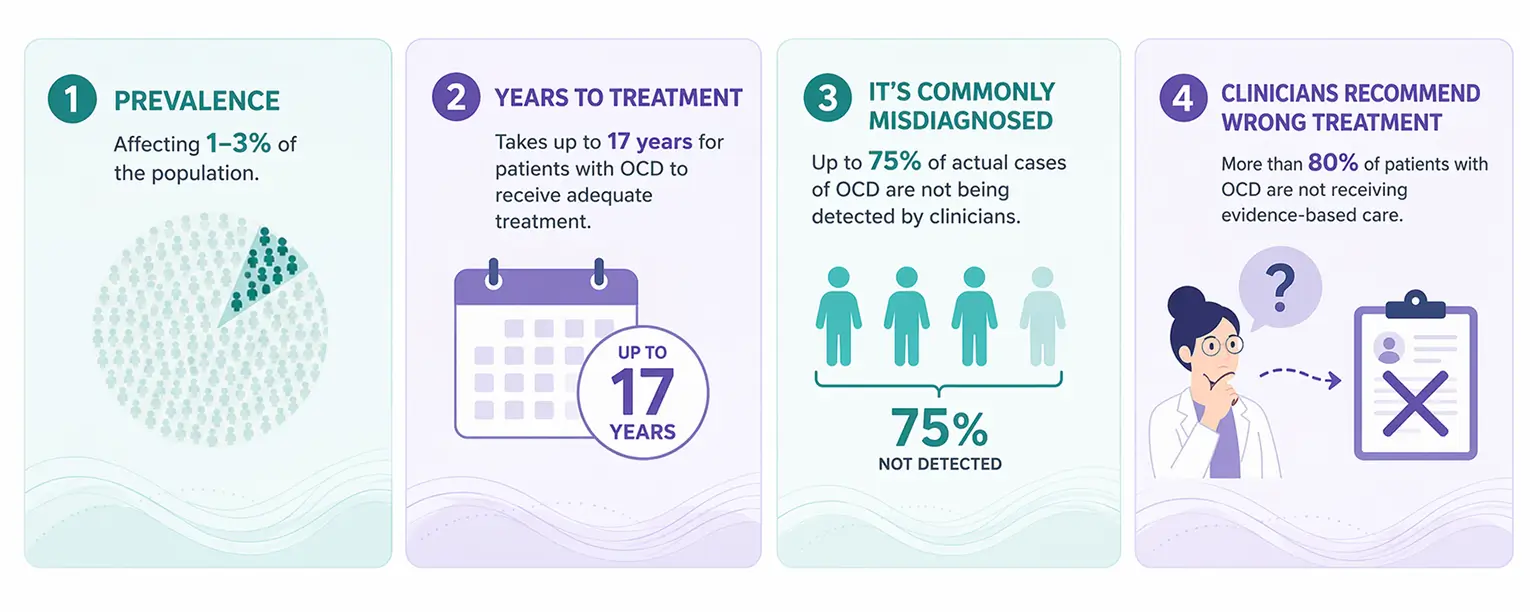
Obsessive-Compulsive Disorder (OCD) is a common mental health condition characterized by obsessions, compulsions, or both. Affecting approximately 1-3% of the population, OCD can cause significant distress and impairment across multiple areas of life.
Healthcare and mental health professionals are likely to encounter individuals affected by OCD, making a basic understanding of the condition important for early recognition, accurate conceptualization, and appropriate support.
What Is OCD?
OCD is characterized by obsessions, compulsions, or both.
Obsessions are recurrent and persistent thoughts, images, urges, or impulses that are experienced as intrusive and unwanted and typically cause significant anxiety or distress.
Compulsions are repetitive behaviors or mental acts that an individual feels driven to perform in response to an obsession or according to rigid rules. These behaviors are often intended to reduce anxiety, prevent a feared outcome, or create a sense of certainty.
Although obsessions and compulsions can take many forms, the underlying processes that maintain OCD are often remarkably similar.
Understanding the OCD Cycle
One of the most important concepts for professionals to understand is the OCD cycle.
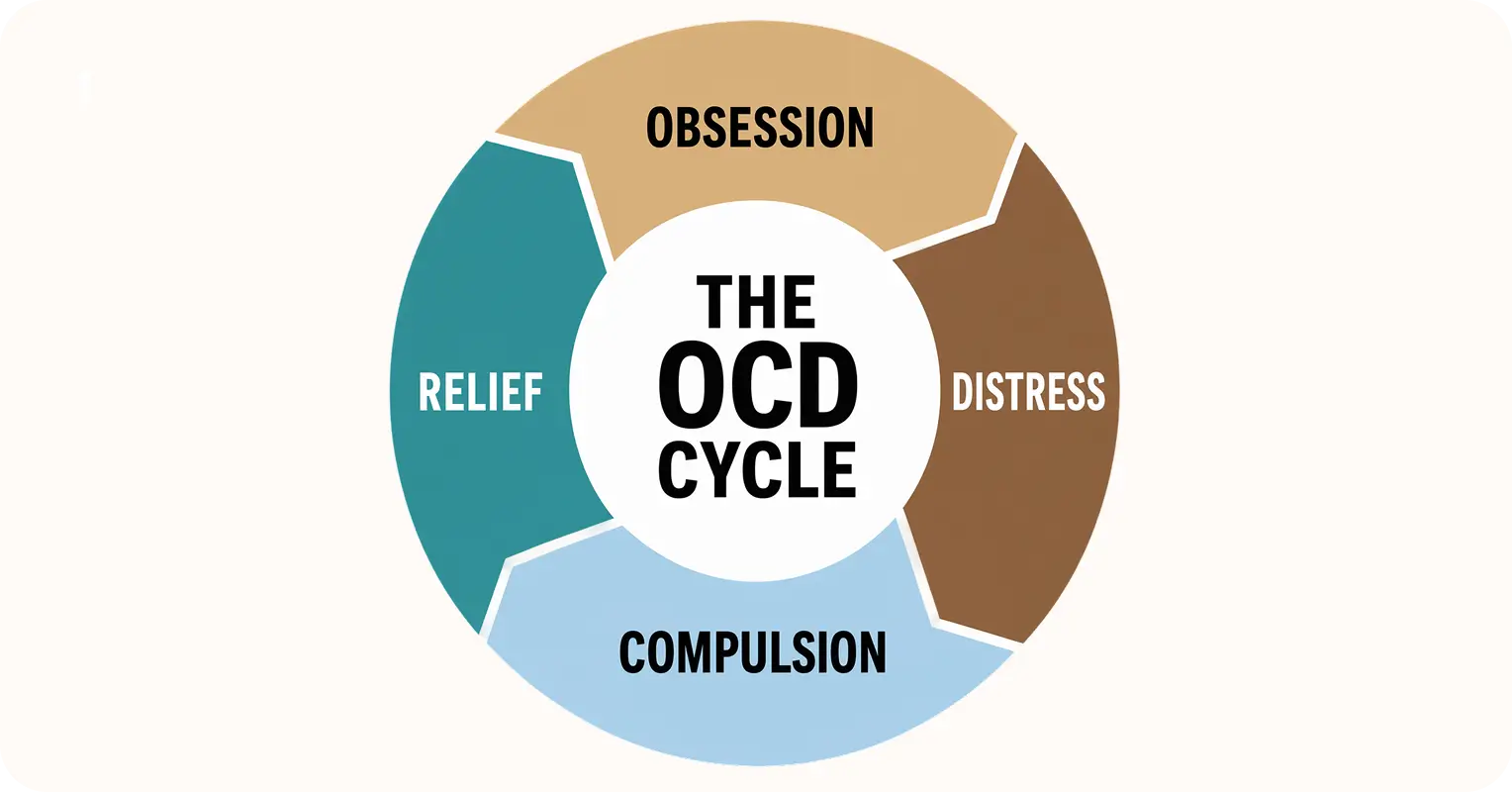
A person experiences an intrusive thought, image, sensation, or doubt. The thought triggers anxiety, uncertainty, guilt, disgust, or fear. In response, the individual engages in a compulsion, i.e. a behavior they feel compelled to do in order to reduce the distress. Although this may temporarily reduce distress, the relief is short-lived.
Over time, the brain learns that the compulsion was responsible for reducing anxiety. As a result, the urge to perform compulsions becomes stronger, and the cycle continues.
Compulsions are not always obvious. In addition to behaviors such as checking, reassurance seeking or washing, many individuals engage in mental compulsions, including analyzing, mentally reviewing, or seeking certainty.
How OCD Presents in Practice
The content of obsessions varies considerably between individuals. OCD is often mistakenly associated only with cleanliness or organization, despite many individuals experiencing obsessions unrelated to contamination.
Common themes include:
- Contamination and illness concerns
- Fear of causing harm
- Excessive responsibility
- Relationship doubts and uncertainty
- Religious or moral concerns (scrupulosity)
- Sexual intrusive thoughts
- Health-related fears
- Existential concerns
Although these themes may appear very different on the surface, they are often maintained by the same cycle of intrusive thoughts, distress, compulsions, and temporary relief.
Professionals may observe:
- Excessive reassurance seeking
- Repeated checking behaviors
- Avoidance of situations, objects, people, or activities
- Difficulty tolerating uncertainty
- Repetitive questioning
- Significant guilt, shame, or self-doubt
- Time-consuming mental review processes
Individuals may not voluntarily disclose symptoms due to embarrassment, fear of being misunderstood, or concerns about how their thoughts will be interpreted.
Differential Considerations
OCD may sometimes be confused with:
- Generalized Anxiety Disorder (GAD)
- Health Anxiety
- Obsessive-Compulsive Personality Disorder (OCPD)
- Psychotic disorders
- Autism-related repetitive behaviors
- Eating disorders
Careful assessment is important because the presence of repetitive thoughts or behaviors does not automatically indicate OCD. Understanding the function of the behavior, the associated distress, and the individual's level of insight can help inform accurate conceptualization.
Evidence-Based Treatment Approaches
Several interventions have demonstrated effectiveness in the treatment of OCD.
Exposure and Response Prevention (ERP) is considered the gold-standard psychological treatment and involves gradually confronting feared thoughts, situations, or triggers while resisting compulsive responses. Over time, individuals learn that anxiety can decrease without performing compulsions and that feared outcomes are often less likely than anticipated.
Cognitive Behavioral Therapy (CBT) may help individuals identify and respond differently to unhelpful beliefs and interpretations that contribute to OCD symptoms.
Acceptance and Commitment Therapy (ACT) is increasingly being integrated into OCD treatment and focuses on helping individuals develop greater psychological flexibility and respond differently to intrusive thoughts and uncomfortable emotions.
Medication, particularly selective serotonin reuptake inhibitors (SSRIs), can also be beneficial for some individuals and is often used alongside psychological treatment.
Effective treatment focuses not on eliminating intrusive thoughts but on changing how individuals respond to them.
Free tools for your patients
Learn about our personalized online therapy program, which empowers you to retrain your brain and find freedom from OCD.
What Professionals Should Know
Perhaps one of the most important things professionals can understand is that OCD is not simply a problem of irrational thinking or a lack of willpower.
Individuals with OCD are often highly aware that their fears may be exaggerated, yet they continue to experience significant distress and powerful urges to engage in compulsions. By the time many seek support, they may already feel ashamed, frustrated, or exhausted from years of struggling with symptoms.
It is also important to recognize that intrusive thoughts do not reflect a person's intentions, desires, values, or character. In fact, individuals with OCD are often distressed precisely because the content of their obsessions conflicts with what matters most to them.
A curious, compassionate, and non-judgemental approach can make a meaningful difference.
Understanding that compulsions often serve as attempts to reduce distress, and that uncertainty lies at the heart of many OCD presentations, can help professionals respond more effectively and support recovery.
Professionals should also be mindful of the role reassurance can play in maintaining OCD. While offering empathy and validation is important, repeatedly providing certainty about feared outcomes may unintentionally strengthen the cycle of obsessions and compulsions.
Final Thoughts
OCD is a common, complex, and frequently misunderstood condition. Although symptoms can be highly distressing, effective treatments are available, and recovery is possible.
Professionals across healthcare and mental health settings are uniquely positioned to recognize symptoms, challenge misconceptions, reduce stigma, and support access to evidence-based care. Greater understanding of OCD can contribute to earlier identification, more compassionate conversations, and improved outcomes for those living with OCD.
Refer patient to StopOCD
Our treatment model is rooted in evidence-based approaches for OCD and delivered by therapists with extensive experience.
References
- American Psychological Association. Obsession. APA Dictionary of Psychology. https://dictionary.apa.org/obsession
- American Psychological Association. Compulsion. APA Dictionary of Psychology. https://dictionary.apa.org/compulsion
- Obsessive-compulsive disorder. StatPearls. National Center for Biotechnology Information. https://www.ncbi.nlm.nih.gov/books/NBK553162/
- OCD-UK. Types of OCD. https://www.ocduk.org/ocd/types/
- StopOCD. Understanding the cycle of OCD. https://www.stopocd.com/understanding-the-cycle-of-ocd
- StopOCD. OCD signs and symptoms guide. https://www.stopocd.com/ocd-signs-symptoms-guide
- StopOCD. Understanding the OCD spectrum. https://www.stopocd.com/understanding-ocd-spectrum